
BACKGROUND
Burj El Barajneh is a Palestinian refugee camp (BBC) in Beirut, Lebanon, and the 6th largest of the 12 official campus established after 1948. According the data collected in 2008-2009, it is home to approximately 14,000-18,000 inhabitants over an area of 1.6 km squared, a number that has continued to increase significantly since then. The dire social and environmental conditions faced by Palestinian refugees in Lebanon are recurrently stated to be the most severe in the region, especially due to limitations in economic resources, employment opportunities and basic health services. The United Nations Refugee and Works Agency (UNRWA) is one of the organizations that provide health and educational services to the refugee population. Despite the severe increase in the populace since its founding, the number of schools remains at a standstill, and the effects of this lack of educational support is evident, particularly among the youth.
IDENTIFY THE COMMUNITY PROBLEM/GOAL TO BE ADDRESSED AND WHAT NEEDS TO BE DONE
The population of Palestinian refugees in Burj El Barajneh refugee camp has been greatly expanding since its establishment in 1948. After observing a high drop-out rate, and high levels of indicators of mental ill-ease among youth, an intervention called “Qaderoon” (Arabic for “We are capable”) was developed, implemented and evaluated in partnership with a community coalition. The aim of the year-long social skills building intervention was to promote positive mental health of the refugee children and increase attachment to school. In order to reach these goals, practitioners developed an evidence-informed intervention that included activities for children, parents and teachers and focused on skills such as improving communication skills, problem-solving skills, and relationships.
ASSESS THE LEVEL OF THE PROBLEM OR GOAL
The Burj el Barajneh camp, located in the southern suburbs of Beirut, is the 6th largest of the 12 official camps. Palestinian refugees in Lebanon have the worst living circumstances of any of the Palestinian refugees in the Arab region (prior to the Syrian crisis that began in 2011), with state-imposed restrictions and very limited human rights. Although education is provided by the United Nations Works Agency, lack of access to work opportunities, as well as crowded classrooms due to underfunding and an expanding population results in many children dropping out of school around 14 years of age. A household survey conducted in 2003, among 13-19 year old unmarried youth living in the camp indicated that 45% were out of school, ands over a quarter (27%) were working. Indicators of mental ill-ease included the occurrence of stressful life events, such as a death in the family over the course of the past year (42%) having a family member in the hospital (67%) and having a parent who had to repay a loan (48%). 67% of youth worked more than 40 hours a week, and 90% earned less than 75,000 LL a week (1$=1500 LL). Only 13% of youth surveyed felt their life would substantially improve in the future, and 68% stated they had fewer opportunities than others in their same age group in Lebanon. Finally, 94% reported they trusted few or no people around them.
DESCRIBE THE PRIORITIZED GROUPS TO BENEFIT AND THOSE IMPLEMENTING THE INTERVENTION
Though the survey was conducted with 13-19 year olds, a community coalition prioritized primary prevention. The prioritized groups to benefit were therefore children ages 11-14 years old who were attending UNRWA schools in 5th and 6th grade and living in the camp. The implementation team consisted of a master trainer, 6 facilitators, and 23 youth mentors. The youth mentors—who all lived in or around the camp and were already part of/familiar with the community—were recruited through NGOs working in the camp and who were members of the Community Youth Coalition (CYC), a group established to guide the development, implementation, and evaluation of this intervention. In that sense, they were a very important part of the implementation team in that they acted as the liaison between the facilitators and the children while they assisted the former in all aspects of the intervention sessions and evaluation process. The master trainer was responsible for supporting the adaptation of the intervention to the context, conducting the pilot sessions, and training and selecting the youth mentors and facilitators, who were chosen based on their prior experience working with children of the similar age groups. The master trainer also had the responsibility of implementing the sessions, completing the process evaluation forms and documenting the changes to the sessions and the reason behind the changes. A field coordinator from the CYC handled the logistics of the intervention, as well as upheld a close relationship with community, family members, and schools.
INDICATE HOW YOU WILL OBTAIN CLIENTS’ INPUT
The Qaderoon intervention was based on data gathered about unmarried young people aged 13-19 years in the BBC but led to the implementation of an intervention for 11-13 year olds. Three phrases guided the development of the logic model for the intervention. The first is described here, others later in this text.
The first was an exploratory phase, and the bulk of it was aimed at obtaining the input from the community. It consisted of a needs assessment (conducted during the spring of 2003) with the objective of assessing youth social and health issues using several data collection methods. Youth ages 13-19 years old who had never been married were interviewed face-to-face after receiving consent from both them and their parent(s)/guardian(s). The results indicated that the youth surveyed were disadvantaged (see above). Focus group discussions were also conducted with male and female younger and older youth to explore the survey results in greater depth and to help prioritize youth issues. These focus groups led to youth creating and practicing short plays that showcased their prioritized issue, and subsequently presenting them to an audience of the CYC and other adults from the community.
The exploratory phase also included conducting focus groups with mothers and teachers of youth in order to gain their perspective on youth health and social issues. Parents stated that youth have no guarantees due to their difficult socio-economic circumstances, lack of financial opportunities, and disengagement with the school system. Their daily life pressures inside and outside the house also affected their mental health. Teachers also discussed their own personal situations of being underpaid and having to work double-shifts, as they come from the same very difficult environments that the children come from. Training workshops that they attended were often not applicable to their classroom circumstances, and the relationships between them and the students were not strong.
ANALYZE THE PROBLEM OR GOAL TO BE ADDRESSED BY THE INTERVENTION
The exploratory phase led to a lot of data being collection. The problem identification phase (phase 2 of the logic model) then began. Based on all this data, information obtained was categorized into main themes versus determinants. Five main themes emerged: mental health, violence, school drop-outs, smoking, and use of drugs. With the CYC, each was ranked according to size, seriousness, effectiveness of solution, as well as acceptability to the community, feasibility, and legality. School drop-out and mental health received the highest ranking and were thus selected as primary outcomes for intervention. The choice was made to focus on positive mental health defined as “a person’s ability to cope with adversity, and avoid breakdown or diverse health problems when confronted with adverse experiences” (Korkeila 2000).
Determinants of mental health and drop out were reviewed in the academic literature. Subsequently, locally specific determinants identified from the survey, from the focus groups, or from the experience of NGOs working in the camp were added to the problem analysis. These determinants spanned various ecologic level from individual, to interpersonal (peers, families) to organization (schools), and to those relevant to the larger environment (context of Lebanon and the camp).
Based on the acknowledgement that root social and political determinants were impossible to change in the short term, a decision was made to focus only on the proximal determinants (individual, interpersonal, and organizational). Within this list, those perceived to be amenable to intervention were selected (see objectives below).
SET GOALS AND OBJECTIVES FOR WHAT "SUCCESS" WOULD LOOK LIKE
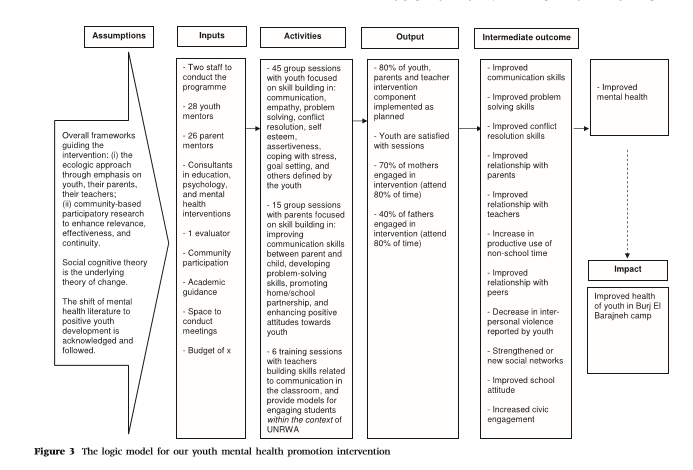
Goals of the program included promoting mental health of refugee children and increase their attachment to school through social skill-building engaging sessions. Objectives included improving communication skills, problem-solving skills, conflict-resolution skills, improving self-esteem, and building relationships.
IDENTIFY AND ASSESS “BEST PRACTICES” OR “EVIDENCE-BASED INTERVENTIONS”
Based on the desired objectives, the team began searching for evidence-based interventions. Specific evidence-based interventions were selected by the CYC based on the following criteria:
The outcome measure was related to mental health or positive youth development; the target age group was appropriate. With respect to age group, mental health issues become especially relevant in this context at age 14, large numbers of Palestinian refugee children drop out of school. The CYC had emphasized the importance of a preventive intervention. Therefore, the age group of 10–14 years was selected as ideal for the intervention; The intervention was intended for a universal (rather than targeted) audience; The length of the programme; The programme involved parents and/or teachers; The setting of the programme was in school or the community (rather than in a clinical setting); The main activities of the programme fit the identified determinants; and The programme was perceived to be adaptable to the context of the camp.
HOW WAS THE ACTION PLAN FOR THE INTERVENTION DEVELOPED?
Selected interventions were summarized based on the criteria described above, and placed on large sheets of paper and hung on the wall. CYC members then circulated and read each of the interventions (see figure 1). Subsequently, a long discussion took place to assess the fit of each with the context based on the experience of the CYC members. This interface of evidence with lived experience resulted in the selection of three evidence-based interventions as most appropriate to the context: Stress Inoculation Training, Improving Social Awareness and Social Problem Solving, and Positive Youth Development Programme. The manuals of these interventions were requested and received from the organizations. As these interventions collectively included activities addressing the identified determinants, the sessions in each were added to estimate the scope of our intervention. Context specific sessions were also added. In keeping with the ecological model, activities with parents and teachers were included.
WAS THE INTERVENTION PILOT-TESTED ON A SMALL SCALE?
Ten sessions were pilot-tested with youth of the same age group recruited from schools in another camp, and changes were made accordingly. The pilot involved the implementation of 20% of the intervention, and the results suggested that procedures needed to be tweaked in order to allow for child privacy when assessing. The pilot session also provided strong feedback in regards to the session length and cognitive level of activities. The use of qualitative methods during this phase was crucial to understanding the intricacies of implementation to achieve objectives and impact youth health.
SPECIFY THE CORE COMPONENTS AND ELEMENTS OF THE INTERVENTION
The core components of the intervention included:
- 45 sessions with youth aged 10-14 years (in grades 5 and 6)
- 15 sessions with parents
- 6 workshops with teachers
The intervention is described in detail in the logic model below.
IDENTIFY THE MODE OF DELIVERY THROUGH WHICH EACH COMPONENT AND ELEMENT OF THE INTERVENTION WILL BE DELIVERED IN THE COMMUNITY
The skills-building sessions for youth were interactive and conducted during out-of-school hours but within school premises. A whole floor (5 rooms in total) was utilized. The intervention period lasted from August 2008 until May 2009. It began in the summer, with an intensive 2-week intervention (summer phase), and continued on during the academic year, taking place on Fridays and during school holidays until May 2009 (fall phase). The youth convened in classes set up either with round tables, or in semi circles or on the floor to create an atmosphere of trust, to facilitate sharing and to eliminate sense of hierarchy.
INDICATE HOW THE INTERVENTION OR “BEST PRACTICE” WAS ADAPTED TO FIT THE NEEDS AND CONTEXT OF YOUR COMMUNITY
When the intervention was still being developed, cultural adaptation was required, because there were issues specific to Arab youth and refugee youth. The process was carried out by a graduate student studying psychology, who was a member of the CYC with background experience in education in the camp with youth. Another young person with a degree in social work and sociology also aided the process.
Some key principles were agreed on: to focus on terms and expressions used by youth in their context, interactive activities rather than lectures; to decrease the need for writing since writing skills were not properly developed; less focus on introspection due to its not being common in the culture and more on collective activities focused on social and cognitive skills. Gender issues needed to be considered, as the community was conservative and girls and boys are segregated in school; consider the use of art and other forms of expression; extend the timing of activities to allow for enough exposure to concepts that are not as common in our context.
With these principles in mind, activities were adapted. Each session began by identifying the session objective, followed by a detailed description of activities to meet the objectives and time allocated to each.
The issue of mixed gender groups was discussed at length with the CYC. It was concluded that, despite the conservative nature of the community, mixed gender groups were acceptable when the intent was educational and to serve the community.
When the intervention was being implemented, facilitators and mentors noted that the children would, at times, have short attention spans. Energizers and songs to get them back on track were developed and used as needed. Several issues related to the unique culture and context arose and had to be dealt with such as seating arrangements of girls and boys and specific topics for role plays. The presence of youth mentors greatly facilitated these decisions. A reward system (stars) was created to make sure ground rules were followed by the children. Weekly discussions between facilitators were held, and changes in activities were made accordingly.
Parents were often a barrier, and interviews with them quickly concluded that it was either because they (parents) were not aware of when the sessions were being held, and also that they did not see a lot of educational value to ‘Qaderoon’ and preferred to have their children study at home. This was met with the creation of English reading sessions to increase the perceived educational value of the program. Monthly schedules were also sent home with children so that the parents could know when the sessions were taking place. The presence and respect of CYC members in the community also led to the cooperation of parent, who would vocalize their thoughts and feelings about the program which would later be discussed at meetings. These discussions indicated great community support for the ‘Qaderoon’ intervention and perceived impact on social skills of participating children.
IMPLEMENT THE INTERVENTION, AND MONITOR AND EVALUATE THE PROCESS AND OUTCOMES
A thorough process evaluation was implemented during the intervention measuring reach, dose delivered and received, satisfaction and fidelity. The process evaluation indicated that session objectives were successful and that specific session activities were applied accordingly. Children had very high satisfaction with the sessions. With respect to dose delivered, for the summer sessions, the percentage of activities implemented (to an extent ranging between 76 and 100%) was reported as 91.2% by facilitators and 81.8% by observers while for the fall sessions, they were reported as 79.4% by facilitators and 71.7% by observers, respectively. As for fidelity (defined as sessions where all activities were implemented as planned), the results show that overall 78% of the activities were fully applied. Finally, the results indicate that in the summer session, in all sessions and groups combined, 90.4% of children chose a happy face to express their rating of the session, as opposed to 87.4% in the fall session.
Figures:
Figure 1-- CYC members discussing potential intervention.
Each flip chart paper on the wall describes one of the evidence-based interventions found in the literature. The CYC members rotated to read ten of these sheets and discussed relevance to the context.


Photos from Qaderoon:




Contributed by Leah Soweid, American University of Beirut, Intern with the Community Tool Box.